|
|
| |
ARTICLES
History The End-to-side Neurorraphy
Dr. Walter Francis Huaraca.
Plastic Surgeon - microsurgeon.
Specialized in Brazil.
Prof. Dr. Fausto Viterbo.
Head of service discipline of Plastic Surgery - Microsurgery of the
Paulista State University, Botucatu, Brazil.
Dr. Jacqueline Freire Freire.
Resident clinical Samborondon Kennedy
Sumary:
The termino-lateral neurorrhaphy (TLN) was taken up by Dr.Fausto
Viterbo in the year 1996 in their experimental work doctoral named
as latero-terminal neurorrhaphy experimental study in rats and found
that this is a new technique, safe and functioning, electrical
stimulation leads, allows passage of axons to regenerate nerve
sutured laterally and maintains the corresponding trophic muscle.
The
presence of the epineurium does not prevent axonal regeneration or
the passage of electrical stimulation. Completely changed the
concepts which had hitherto existed, that axons do not penetrate the
membranes of connective tissue endo-peri-epineurium. The results
demonstrate the possibility of using this type of neurorrhaphy, in
recovery of nerve injury, when there is only a distal end, being
able to get to this point, at the expense of a nerve without
compromising full functional, this technique has been used
clinically
by Viterbo, from 1,993 in
a series of peripheral nerve disorders such as facial paralysis,
paraplegic patients, brachial plexus palsy through direct
myoneurotization, among others.
Key
Words:
Nerve
Injuries, End-to-side neurorraphy, Microsurgery, Tops Model.
Introduction:
Until the late eighteenth century it was believed that the
nerves do not regenerate. Throughout the nineteenth century, the
debate about regeneration, where Waller defended the fact that
after a section of a nerve axons in the proximal segment were
connected to the cell body and therefore remained viable, and
distal segments degeneraban.1
The technical principles of surgical repair of peripheral
nerves, are based on observations of Waller (1851) in respect of
the regeneration of the distal end of the projections
(Sprouting) axoplasm from the proximal end of sectioned nerves (Terzis,
1979). 2
Since Saliceto William (1210-1277) made the first neurorrhaphy
in Poland, in 1977 Daniel and Terzis used microsurgery to attach
the ends of severed nerves in various ways (epineural,
perineural, interfacicular all, so the term - terminal ) .2
At present up to 1cm nerve regeneration is a reality techniques
using biosynthetic materials, biodegradable as collagen mesh-polyglycolic
acid, poly-3-hydroxybutyrate (PHB) .3 and the latest in
technology, the use of stem cells ( stem cell) of ectodermal
(hair follicle), as pioneers in cellular engineering, UEA Japan,
Taiwan, France, Brazil, where they run every day new scientific
research projects.
History of the End-to-side neurorrhaphy:
The accounts of the termino-lateral neurorrhaphy (NTL) began in
the nineteenth century.
In 1876 Depres, story the repair of the median nerve through the
distal insertion of the lateral nerve ulnar.3
In 1889 Kennedy story, the treatment of a patient with facial
spasm through end-to-side neurorrhaphy, the author performed the
facial nerve section and the distal end joined to the lateral
aspect of the hypoglossal nerve. This case was published in
1.901.3
In 1895 Ballance also repair facial nerve suturing the distal
end after being severed to the lateral accessory nerve palsy
treatment facial.3, 4
In 1903 Harris & Low repair an injury to the upper trunk of the
brachial plexus through the rehabilitation of injured nerve
distal lateral face of the seventh root cervical.3
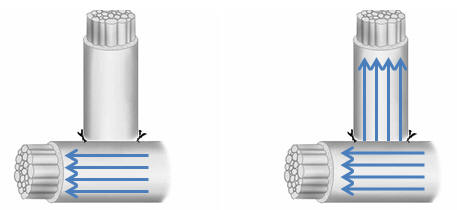
Several authors used the termino-lateral neurorrhaphy getting
good and bad results, for this procedure performed incision in
the donor nerve, the epineurium just to keep safe on the
opposite side to the neurorrhaphy (Sherr 1906) Figure 1.
|
 |
|
Figure 1: Diagram of the lateral neurorrhaphy term used
in the years 1876 -1927 |
The results were not encouraging neurorrhaphy is leading to
Babcock in 1927 to contraindicate its use, due to poor results,
due to the large opening in the epineurium of the donor nerve,
which caused significant damage to structures is innervated
according to the description in 1.906.3,5 Sherrem
This determination led to the abandonment of this technique for
several decades until it was revived by Dr. Fausto Viterbo in
1992 in his doctoral thesis known as latero-terminal
neurorrhaphy experimental study in mice, developed at the
University Estadual Paulista, Botucatu (UNESP) - Brazil 2
Materials and Methods:
Mice were used 40 Wistar, male, weighing between 225-280gramos
rough, raised in the Central Vivarium Universidade Estadual
Paulista (UNESP) Botucatu campus.
The animals were divided into 3 groups with 20 mice in group A,
group B-C with 10 animals each.
Results:
In this first work, Viterbo did not remove the epineurium of the
nerve that was obtained with a termino-lateral neurorrhaphy
pure. Chart 2.3 axons grow laterally which guarantees maintain
tropism muscular.6
|
 |
|
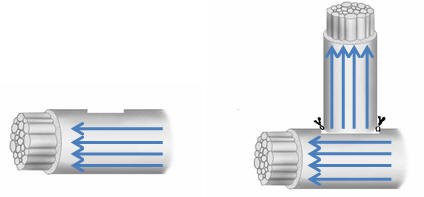
Graph 2: Diagram of the lateral end neurorrhaphy pure
(NTL) used by Viterbo.
Figure 3: Diagram of the (NTL) after 6 months showed
growth of nerve axons from the donor to the distal end,
published by Viterbo in 1992. |
The animals in group A, showed the fibular nerve sectioned and
sutured laterally to the distal tibial nerve without removal of
epineuro6 intact, Figure 4.
|
 |
|
Gráfico4: fibular nerve section, and the distal end is
sutured with NTL in the lateral tibial nerve. |
The test morphological and electrophysiological observations
were verified by the presence of regenerated myelinated fibers
in most animals.
In other work, using the same experimental model plus the
removal of segment-8 Graphic perineuro.7. 5.6
|
 |
|
Figure 5: Schematic of termino-lateral neurorrhaphy
(NTL) with minimal removal of the epineurium, used by
Viterbo. Figure 6: Schematic of the (NTL) after 6 months
showed growth of nerve axons from the donor to the
distal end, published by Viterbo in 1994. |
Another difference found, both morphologically and
electrophysiologically, was the growth of donor nerve axons to
the distal fibular nerve, not donor nerve injury present in its
territory of innervation, thus becoming, any potential nerve
donor nerve. The discovery deep doubts, due to the limited
knowledge at that time, the axons could never cross the
membranes of tissue involved, namely: endoneurium, perineurium,
epineurium. Meanwhile various experimental changed these
resistances. Photos 6-8: 6.2.
DISCUSSION:
In the published works of Viterbo, in the NTL without removal
and removal of the epineurium were similar in their results, ie
found no statistical difference in the size and number of axons,
and therefore the removal of the epineurium or not does not
imply in the transmission of healthy nerve axons toward the
distal end. 2-15.
The indication of the end-to-side neurorrhaphy, occurs when the
proximal end of the injured nerve is not available for carrying
out the traditional repair-terminal terminal and can use
multiple grafts without affecting healthy nerve function.
The author uses this type of neurorrhaphy without removal of the
epineurium in all 16,17,18,19,28,29,30 microsurgery.
CONCLUSIONS:
1 .- In this comparative study, Viterbo, carried to term-lateral
neurorrhaphy with or without removal of the epi-perineurium. 6-8
2.-The histological results 6 months after surgery, by slitting
the site of termino-lateral neurorrhaphy, and nerve
cross-receptor, were found lateral sprouting epineurium and
perineurium disappearance of the suture site in both groups.
Photo 2.6.
3.-They found no differences in morphological and
electrophysiological characteristics in the groups studied. 2
4 .- The term-side neurorrhaphy is functional electrical
stimulation leads, allows the passage of axons to regenerate the
nerve sutured laterally and keeps trophism of muscle. Photo:
7,8,9.
5 .- The presence of the epineurium does not prevent axonal
regeneration, or the passage of electrical stimulation. 2-15
6.-These results demonstrate the effectiveness of this type of
neurorrhaphy in the recovery of nerve injury when only provides
end-distal reinnervation may be obtained from this end (distal)
at the expense of compromising functionally integrates nerve.
Clinical Applications:
This technique is being used by Viterbo from año1.993 in the
treatment of peripheral nerve disorders like facial paralysis
with excellent results, as in paraplegic patients as treatment
of pressure ulcers, restoring sensitivity to soft tissue,
another applications such as direct muscle neurotization (mioneurotización),
which involves implanting one end of the nerve or nerve segment
between a paralyzed muscle fibers, being shown to restore muscle
function only when the trauma or injury leads to loss of
neuromuscular function (Becker et al, 2002) this technique
provides good results in brachial plexus injuries. 16-30.
Another application would be looking for penis amputees who
performed phalloplasty. This technique opens the possibility of
placing a nerve graft at the neo-glans with the hope of
restoring sensitivity.
It could also be used in patients with urinary incontinence.
This technique would be based on placing a nerve graft at the
level of the bladder in order to return the voluntary act of
urination.
REFERENCES:
1.Sociedad Plastic and Reconstructive Surgery Year 2000 1st
edition chapter 59
2. Viterbo F. Latero-terminal neurorrhaphy, no experimental
estudo time. UNESP Botucatu, 1992. p.198. Tese (Doutor) -
Faculdade de Medicina, Universidade Estadual Paulista.
3. Susan Mueller. Axonal regeneration from the intact nerve to
partially injured nerve neurorrhaphy using the term - side-trabalho
experimental brachial plexus while no UNESP Botucatu 2.008.Tese
(Doutor), Faculty of Medicine, Universidade Estadual Paulista.
4. Ballance CA. Remarks on the operative Treatment of chronic
facial palsy of peripleral origen.BMJ 1903, 2: 1009-1013.
5. Standard technique for WW.A Babcock Operations on peripheral
Nerves with Special reference to the closure of large gaps. Surg
Gynecol Obstet 1927; 45:364-78.
6. Viterbo F, Trindade JC, Hoshino K, Mazzoni A neuroraphy
Latero-terminal removal of the epineural Without Sheater.
Experimental study in rats. Rev Paul Med 1992, 110: 267-275.
7. Viterbo F, Trindade JC, Hoshino K, Mazzoni A Two end-to-side
nerve graft neurorraphies and removal of the epineural with
sheath: experimental study in rats. Brit J Plast Surg 1994; 47:
75-80.
8. Viterbo F, Trindade JC, Hoshino K, Mazzoni A. End-to-side
nerve graft neurorraphies and removal of the epineural with
sheath: an experimental study in rats. Plast Reconstr Surg 1994;
94: 1038-1047.
9. Bertelli JA, Santos ARS, Calixto JB. Is axonal sprouting Able
to traverse the conjunctival layers of the peripheral nerve?
Abehavioral, motor, and sensory study of end-to-side nerve
anastomosis. J Reconstr Microsurg. 1996, 12:559-563.
10. Noah EM, Williams A, Fortes W, Terzis JK. A new animal model
to axonal sprouting Investigate after-end-to-side neurorrhaphy.
J Reconstr Microsurg. 1997, 13:317-325.
11. Caplan J, Tiangco DA, Terzis JK. Effects of IGF-II in a new
end-to-side model. J Reconstr Microsurg. 1999, 15:351-358.
12. Mennen U. End-to-side nerve suture in primate (Chacma Baboon).
Hand Surg. 1998, 21:1.
Zhang F, Cheng C, Chin B, et al. Results of termino-lateral
neurorrhaphy to original and Adjacent Nerve. Microsurgery 1998;
18:276-281.
13. Matsuda K, Kakibuchi M, Fukuda K, et al. End-to-side nerve
grafts: Experimental study in rats. J Reconstr Microsurg. 2005,
21:581-591.
14. Papalia I, Geuna S, Tos PL, Boux E, Battiston B, Stagno
D'Alcontres F. Morphologic and functional study of rat median
nerve repair by neurorrhaphy of the ulnar terminolateral nerve.
J Reconstr Microsurg. 2003, 19:257-264.
15. Akeda K, Hirata H, Matsumoto M, et al. Regenerating axons
emerge far proximal to the coaptation site in end-to-side nerve
coaptation Without a perineurial window using a Tshaped chamber.
Plast Reconstr Surg. 2006, 117:1194-1203.
16. Viterbo F. Novo method gives Paralisia tratamento facial or:
o "cross-face nerve" termino-lateral neurorrhaphy com. Rev Soc
Bras Cir Plast Reconst Est 1993, 8: 36-38.
17. Viterbo F, Palhares A, Franciosi LF. Restoration of
sensitivity After removal of the sural nervea New application of
lateralterminal neurorraphy (case report). Rev Soc Bras Cir
Plast Reconstr Est 1993, 8:8587.
18. Viterbo, F. A new method for Treatment of facial palsy: The
cross-face nerve transplantation With End-to-side neurorrhaphy.
(Abstracts) Plastic and Reconstructive Surgery 98 (1): 189,
1996.
19. Viterbo, F. "Transposição orthodromic temporalis muscle for
or give paralisia tratamento Melhor facial.Contribuição for
cosmetic result," as the theme livre appresented not XXXVI
Brazilian Congress of Plastic Surgery. Rio de Janeiro, 16
novembre 1999.
20. Al-Qattan MM. Prevention and Treatment of painful neuromas
of the superficial radial nerve by the end-to-side nerve repair
concept: An experimental study and preliminary clinical
experience. Microsurgery 2000; 20:99-104.
21. Sundin MJ, Quan EE, Saglam O, et al. The use of end-to-side
nerve grafts to reinnervate the paralyzed orbicularis oculi
muscle. Plast Reconstr Surg. 2003, 111:2255-2264.
22. Millesi H. Surgery of post-traumatic brachial plexus
injuries (personal approach in 2003). Plast Mikrochir Handchir
Chir.2004, 36:29-36.
23. Mennen U, Van Der Westhuizen MJ, Eggers IM. Re-innervation
of M. biceps by end-to-side nerve suture. Surg.2003 Hand,
8:25-31.
24. Yamamoto Y, Sasaki S, Sekido M, et al. Alternative approach
using the technique of nerve crossover Combined crossnerve
grafting for reanimation and of facial palsy. Microsurgery
2003, 23:251-256.
25. Frey M, Giovanoli P, Michaelidou M. Functional upgrading of
Partially Recovered facial palsy by cross-face nerve grafting
with distal end-to-side neurorrhaphy. Plast Reconstr Surg.
2006, 117:597-608.
26. Franciosi LF, Modestti C, Mueller SF. Biceps muscle of the
Neurotization by end-to-side neurorrhaphy ulnar and
musculocutaneous Nerves Between: A series of five cases. Ann
Hand Surg. 1998, 17:362-367.
27. Vocho P, Ouattara D. End-to-side neurorrhaphy for defects of
palmar sensory digital Nerve. Br J Plast Surg. 2005, 58:239-244.
28. Viterbo, F. & Faleiros, H.R.P. Transposition of the
orthodromic muscle for facial paralysis, made easy and better.
J. Craniofacial Surg. 2005 Mar, 16 (2) :306-9.
29. Viterbo F, Ripari WT. Nerve grafts paraplegic Prevent
pressure ulcers. J Reconstr Microsurg. 2008, 24:251-253.
30 Viterbo F, The End-to-side Neurorraphy, Past, Present, and
Future, Plastic Sugery 124,351 e, 2009.
|
|
|
|